Abstract
Maintaining an optimal stability (OS) serves as a primary criterion for self-optimization of human locomotion [1], a process whereby adaptations in biomechanics and physiology coincide. It has been suggested that wearable trunk accelerometry (WTA) could be used as an in-field tool to evaluate OS while running [2], yet this theory currently remains untested. Here, we hypothesized that WTA stability measures could be used to evaluate if runners have an OS, and if so, whether OS would be linked to physiological manifestations of fatigue.
MethodsRecreational runners (n=22) participated in a discontinuous incremental running protocol on a motorized treadmill (4min stages; 1min rest periods; starting at 8 or 9km.hr-1; 1.5km.hr-1 speed increments; 1% gradient). Blood lactate was collected before every speed increment using a portable lactate analyzer (LactatePro2, Japan), and onset of blood lactate (OBLA) was defined as >4mmol.L-1. Tri-axial (vertical, mediolateral, anteroposterior) acceleration root mean square (RMS) measures were extracted from gravity-corrected trunk accelerations (Shimmer3, ±16g range, 1024Hz, Ireland). Each axis RMS was normalized to the resultant RMS vector to represent the proportion of acceleration occurring in each axis (i.e., RMS ratio), and calculated over non-overlapping moving average of 10seconds during the entire running protocol (MATLAB 2017b, USA). Linear and quadratic fits were assessed for each RMS ratio using goodness of fit (R2), and comparisons between models were done using paired t-tests. Additionally, paired t-tests and Pearson’s correlations were performed between the time (min) of OS and OBLA.
ResultsOS was identified in all runners using the vertical RMS ratio and thus this measure was used for further analysis (e.g. Fig1). Fitting a curvilinear (quadratic) model to vertical RMS ratio consistently produced significantly higher R2 values than fitting a linear model (mean R2 0.63 and 0.93 for linear and quadratic fits; p<0.01). Time of OS occurred significantly earlier than OBLA (5.9±2.9 min versus 15.8±4.2 min; p<0.05) and was not correlated (r=0.05).
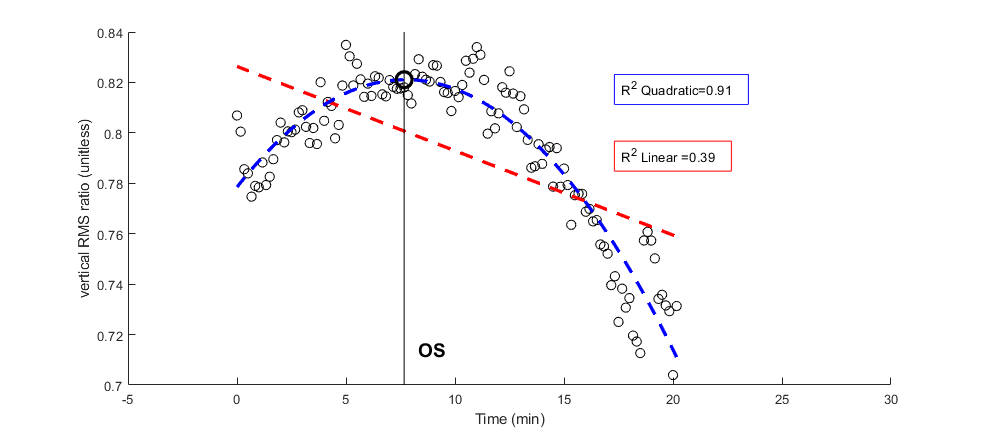
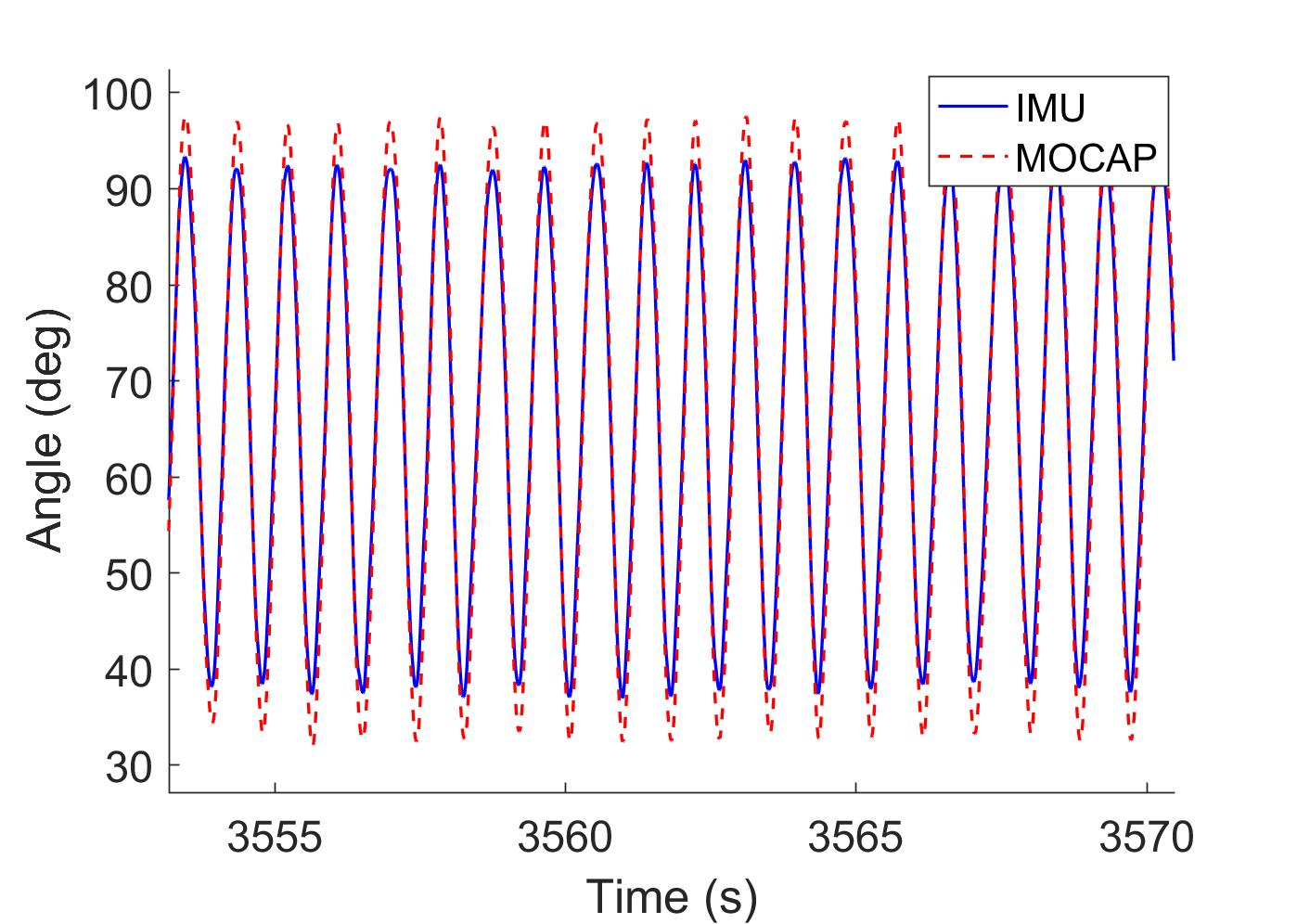
Fig.1: Comparison of linear and quadratic goodness of fit for one representative runner using vertical RMS ratio. Optimal stability optimum (OS) occurred at 7.7min.
DiscussionOur first hypothesis was supported in that runners demonstrated an OS using the RMS ratio measure of vertical trunk accelerations. In contrast to previous research [3], our data suggest that runners self-optimize their stability, possibly due to a combination of preferred speed and fatigue. However, our second hypothesis was refuted since OS was not related to OBLA, indicating that other manifestations of fatigue (e.g., ventilatory threshold) warrant further investigation.
References1. Holt KG, et al., J Mot Behav. 1995;27: 164–78.
2. Schütte KH, et al., J Appl Physiol. 2017; 3–6.
3. McGregor SJ, et al., PLoS One. 2009;4: e7355.
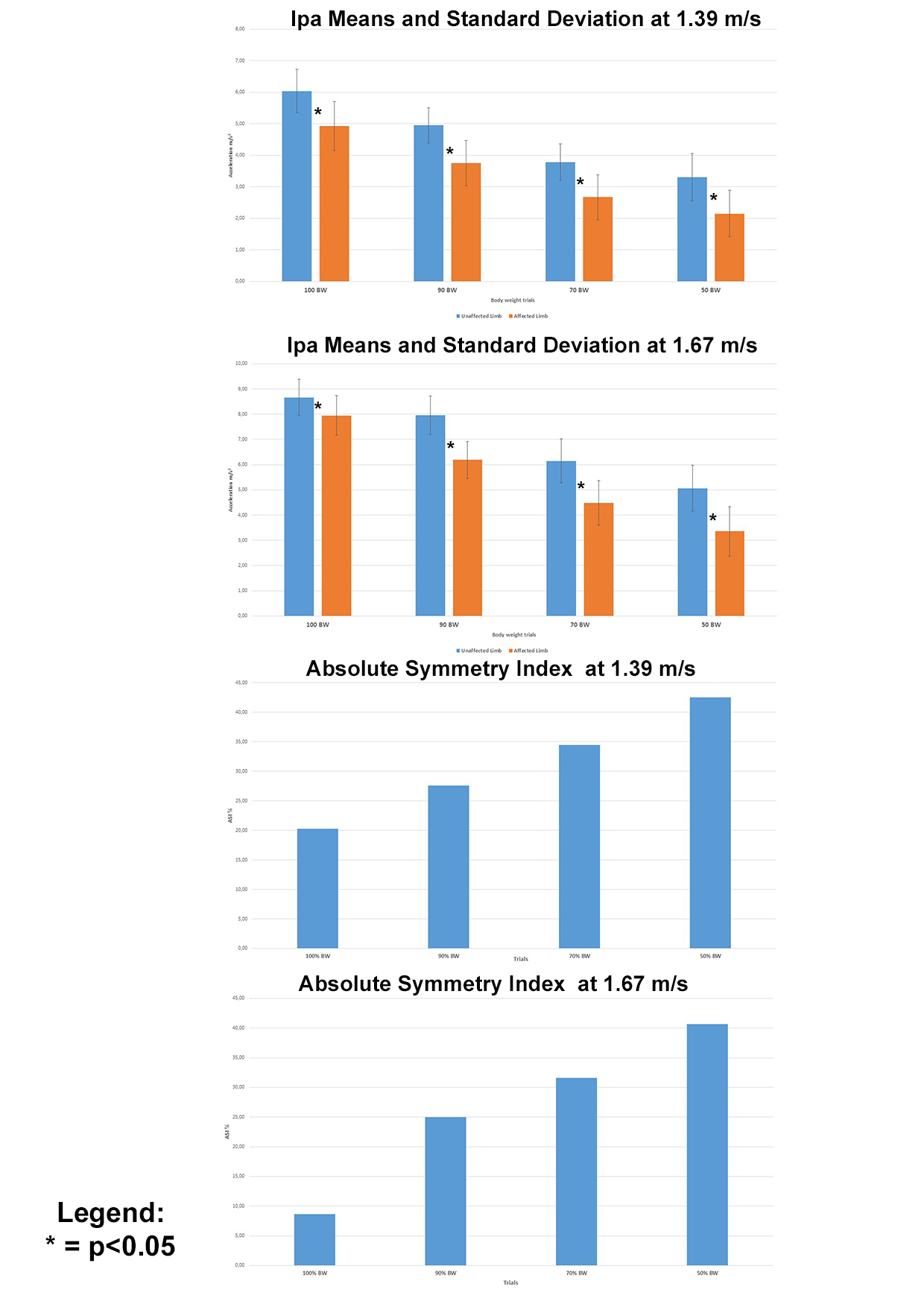
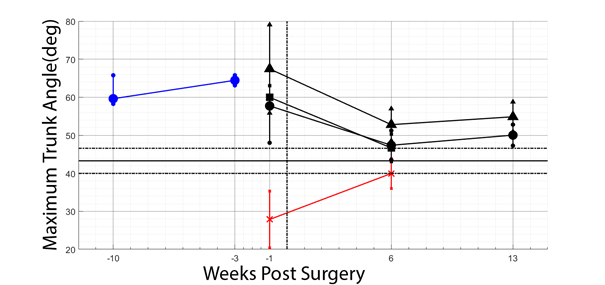
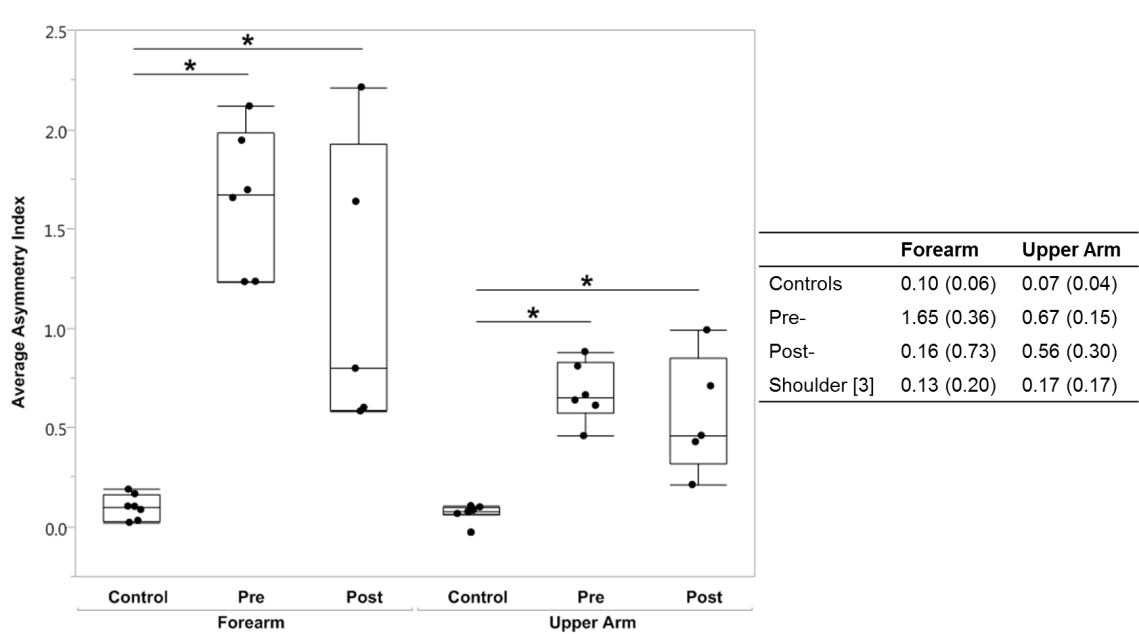 An asymmetry index closer to 0 indicated more symmetry between sides. Control subjects were the most symmetrical. Asymmetry indices for all subjects with BPIs were significantly different from controls (Figure 1). While the asymmetry indices of the post-reconstruction group trended towards control values, they remained significantly different.
An asymmetry index closer to 0 indicated more symmetry between sides. Control subjects were the most symmetrical. Asymmetry indices for all subjects with BPIs were significantly different from controls (Figure 1). While the asymmetry indices of the post-reconstruction group trended towards control values, they remained significantly different.