Primary topic
BACKGROUND
For persons with a lower leg amputation (PwA), walking on uneven ground require compensatory movement strategies, partly caused by limited adaptability of prosthetic components. Walking on cross-slopes, a form of uneven ground, is a situation active PwA face regularly. However, only few studies investigated cross-slope walking of PwA [1-3], and the one that studied adaptations focused on the swing phase on the prosthetic side [3].
AIM
To investigate in more detail the effects of cross-slopes on gait characteristics (in stance and swing phase) of persons with a transtibial amputation (TTA) and compare it with level walking.
METHOD
12 TTA were provided with energy-storage and return feet (ESR) for the time of the study. Level walking and cross-slope walking on 5° and 10° tilted tracks were investigated in a gait lab. Kinematic data were recorded with a Vicon system. A Kistler force plate was embedded in the track to measure the ground reaction forces (GRF). Spatio-temporal and biomechanical parameters (GRF, sagittal ankle and knee angles, pelvis inclination and upper body tilt) were analyzed with respect to situation and side. A repeated measurement ANOVA with post-hoc tests were used to show possible differences to level walking.
RESULTS
Spatio-temporal gait characteristics and GRF showed known differences between prosthetic and sound side but reveled only minor adaptations for the different cross-slope situations. Significant adaptations to the different situations were observed in the sagittal knee and ankle angles, in the pelvis inclination and upper body tilt compared to the level situation. The sagittal ankle angle of the sound side showed a reduced range of motion for Valleyside and an increased one for Hillside while the prosthetic side was unaffected. For the sagittal knee angle, adaptations were observed for the sound and the prosthetic side, figure 1A, which adapt the functional leg length. Pelvis inclination and upper body tilt showed similar adaptations to the cross-slope tilt, figure 1B, which are likely compensation and/or stabilization mechanisms of the upper body.
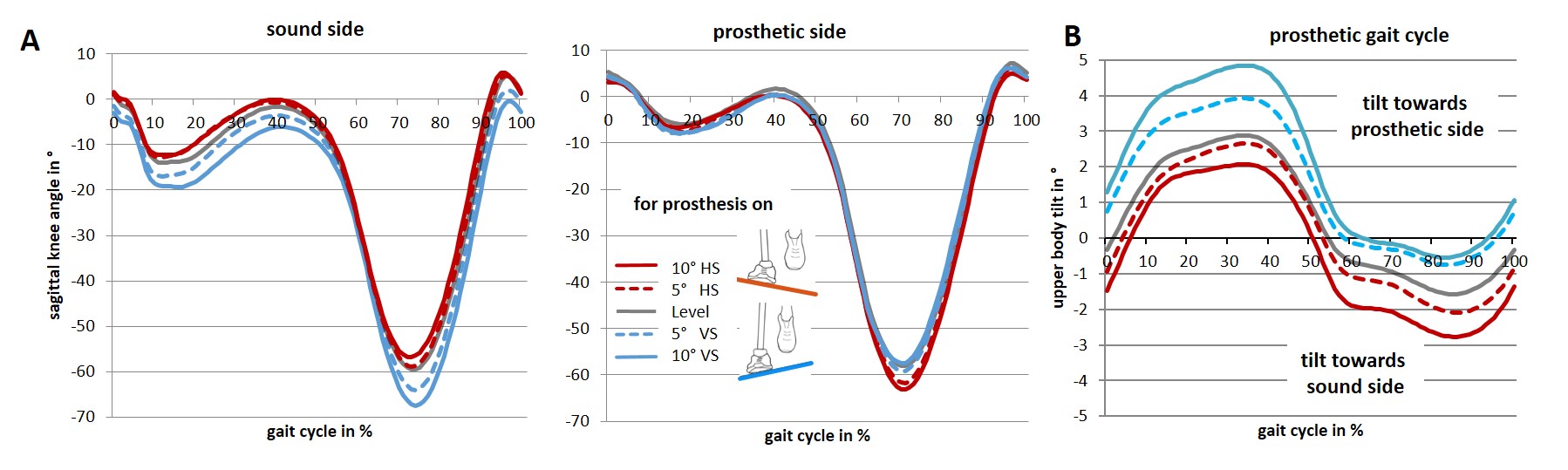
Figure 1: Sagittal knee angle and upper body tilt.
DISCUSSION AND CONCLUSION
Adaptations to the cross-slopes were observed for the prosthetic and sound side in some parameters. Its effect size increased with increasing cross-slope tilt. The results confirm and extend findings of previous studies [3]. However, most observed effects had the same order of magnitude or were smaller compared to general adaptation effects in gait of TTA if compared to controls.
REFERENCES
[1] I. Hak, et al., Arch. Phys. Med. Rehabil. 94 (2013) 2186-93.
[2] I. Starholm, et al., Prosthet. Orthot. Int.; 34(2010) 184-94.
[3] C. Villa, et al., Arch. Phys. Med. Rehabil. 98 (2017) 1149–1157.