Abstract
Objective: Ambulatory tubeless percutaneous nephrolithotomy (PCNL) has been shown to be safe and effective in highly selected patients. However, these selection criteria preclude the majority of patients that undergo PCNL. The objective of our study was to compare complication and stone free rates after ambulatory tubeless PCNL in standard selection criteria vs. extended criteria patients.
Methods: Retrospective review of prospective data on all patients who underwent ambulatory tubeless PCNL at one academic center from 2007-2018. Extended criteria patients were defined as one or more of: Age >75 years, BMI >30 kg/m2, ASA >2, bilateral stones, solitary kidney, transplant kidney, complete staghorn calculi, stone burden >40 mm, multiple tracts, or prior nephrostomy tubes/stents. Primary outcomes were complication rates (Clavien-Dindo classification) and stone free rates (total residual stone burden <3 mm).
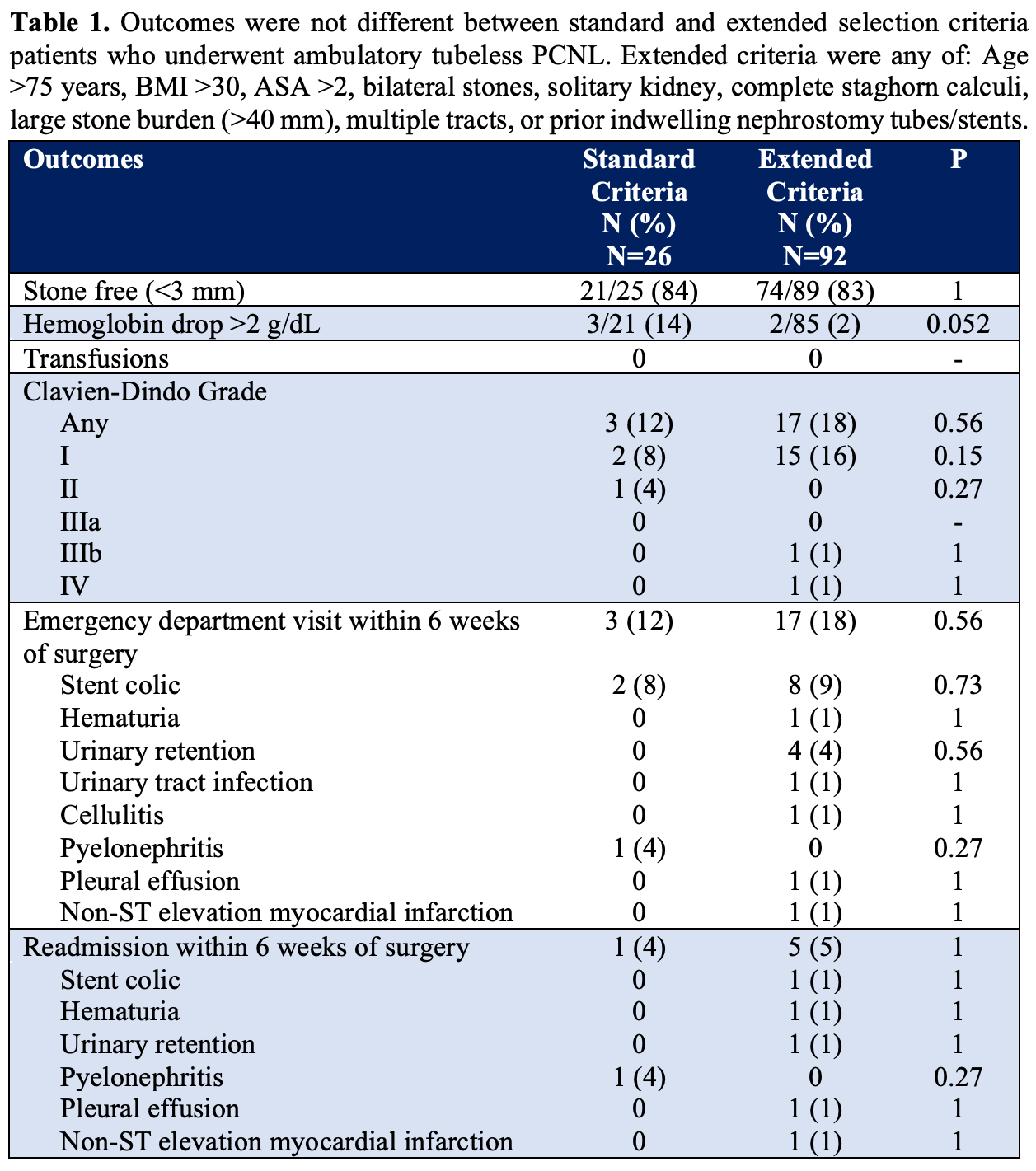
Results: We identified 118 patients of which 92 (78%) met extended criteria. Mean BMI was 31 kg/m2 and 45% were ASA 3 or higher. Mean sum maximum stone diameter was 24 mm. Multiple stones were present in 25%, bilateral stones in 7%, complete staghorn stones in 4%, and pre-existing nephrostomy tubes/stents in 4%. There was no difference in complication (12% vs. 18%, p=0.56), Emergency department visit (12% vs 18%, p=0.56), or readmission (4% vs. 5%, p=1) rates between standard and extended criteria patients respectively. Of the complications, 85% were Clavien-Dindo grade 1. Stone free rates were not different between standard (84%) and extended (83%) criteria patients (p=1). No extended criteria variables were associated with complications in univariate analysis. Stone burden >40 mm (odds ratio [OR] 5.8, 95% confidence interval [CI] 1.4-25.2, p=0.018) and multiple tracts (OR 13.1, 95% CI 1.1-154.7, p=0.041) were associated with residual stone fragments in multivariable analysis.
Conclusions: Complication and stone free rates were not different between standard and extended selection criteria patients undergoing ambulatory tubeless PCNL. This data supports the safety and efficacy of ambulatory tubeless PCNL in patients using extended selection criteria.